Learn about the treatment options for both allergic and invasive aspergillosis.

TREATMENT OF ASPERGILLOSIS
Allergic Forms
The management of allergic forms of aspergillosis may involve several strategies, depending on the particular type of allergic aspergillosis and the stage of the disease. Below are some of the treatments that may be used.
 Medications
Medications
Steroids (corticosteroids)
Steroids are used to reduce inflammation and manage symptoms. They are used to reduce inflammation in various diseases.
Steroids are commonly used medications, but they have to be used in a very specific way. Here are some common tips for getting the best results from steroids:
- Take your medication exactly as prescribed.
- Your provider may encourage you to take the medicine in the morning—sometimes steroids can cause you to become excessively energetic, so it’s best not to take them at night. If you take the medicine at night, you may be too wound up to sleep.
- They can cause indigestion—your provider may want to provide antacid therapy. Take the steroid with food.
- If you are having mood changes—becoming angry, reactive, or hyper—let your provider know. They may adjust the dose.
- Anticipate that your provider will wean you from steroids over a period of time—you should not stop cold turkey (suddenly and completely).
- If you have diabetes, care must be taken in giving you steroids, since they can elevate your blood sugar.
Antifungal Medications
Sometimes antifungals are used along with corticosteroids or instead of corticosteroids for allergic forms of aspergillosis. Your provider will make the best decision for you. For allergic aspergillosis, itraconazole and voriconazole are the antifungal agents used most often. A more detailed discussion of antifungals is included in the Treatment of Invasive Aspergillosis section below.
Other Medications
 Nasal steroids: Nasal spray steroids can be used to reduce inflammation in patients with allergic fungal rhinosinusitis.
Nasal steroids: Nasal spray steroids can be used to reduce inflammation in patients with allergic fungal rhinosinusitis.
Bronchodilators: These are medications to help open the airways and improve breathing. They are used in some of the allergic forms of aspergillosis.
Invasive Aspergillosis
Invasive aspergillosis is a serious condition, so a lot of effort is made to try to prevent it or treat it aggressively. Some general principles apply to management of invasive aspergillosis. These include:

Careful consideration of prophylaxis. Prophylaxis practices vary from provider to provider and from institution to institution. Most providers are careful to only use antifungal prophylaxis in patients who are at very high risk for invasive aspergillosis. Other providers do not use prophylaxis at all for their high-risk patients. Why be so careful with prophylaxis? Reasons include cost of therapy, side effects, the interactions with other drugs, and the problem of antifungal resistance (See Science Sidebar).

Early treatment if possible. Prompt diagnosis and management of invasive aspergillosis improve outcomes. Sometimes, clinicians will treat empirically for aspergillosis, particularly in someone who has long-standing neutropenia (low white blood cells of a specific type) and a fever that has not gone away despite broad-spectrum antibiotic therapy. However, wherever possible, it’s best to test for galactomannan or Beta-D-glucan) to establish a fungal infection in such patients. When therapy is guided by such testing, it’s called pre-emptive and is the preferred approach.

Testing for antifungal susceptibility when treatment fails. Antifungal-resistant aspergillosis is becoming a bigger problem. In Europe, nearly one in five A. fumigatus cases is resistant to azoles, a common type of antifungal medication. In the United States, we don’t think that there is as much of a problem with antifungal resistance in Aspergillus. However, we don’t have great surveillance for this problem, and we have somewhat limited antifungal susceptibility testing. You can ask about antifungal susceptibility testing if the first therapy doesn’t work. See Science Sidebar: Fighting Aspergillus Resistance to learn more.

Addressing pharmacology. Many of the patients receiving antifungal medications for invasive aspergillosis have weakened immune systems or are very sick. These patients are likely to receive other medications that can possibly affect the levels of the antifungal drug. In addition, their kidneys and livers may not be working well. For these reasons, the provider needs to be cognizant of all the factors that could affect the antifungal drug levels. There’s a “Goldilocks zone” with drug levels—too little drug and you don’t get efficacy, too much drug and there can be side effects, the “just right” level is the most effective and safe. For these reasons, providers may use antifungal therapeutic drug monitoring to make sure the drug levels are in the right range.
Science Sidebar:
Fighting Aspergillosis Resistance

Antifungal resistance means fungi can resist or evade the effects of the drugs used to kill them. Some fungi are naturally resistant to certain antifungal medications. So knowing the species of Aspergillus is helpful when planning therapy. But, increasingly, fungi develop the ability to defeat our antifungal medications. How does this happen? Typically fungi get exposure to the enemy (the drug) in a non-lethal situation. The fungi can then develop strategies to evade the enemy in a more lethal situation.
– Agricultural/industrial pesticides. In agricultural or industrial settings, Aspergillus fungi in the environment are exposed to azole compounds in fungicides that are similar to antifungal medications. The fungi can then develop resistance.
– Medical overuse/misuse. Similarly, sometimes fungi are exposed to antifungals and given the opportunity to develop resistance. Overuse/misuse might mean use of antifungals:
- In conditions not caused by fungi
- At too low a dose
- For too long or too short a treatment period
- As prophylaxis in patients who don’t need it.
What can be done?
MyCARE is committed to helping address antifungal resistance in the US and globally. In terms of addressing potential Aspergillus resistance, as a patient you can:
- Find out which genus and species of Aspergillus you have. This is important information your provider should have when selecting the best therapy for you
- Ask about antifungal susceptibility testing if your Aspergillus does not respond to the first therapy given (see “Questions to Ask Your Doctor”)
- Take all of your medications as prescribed.
- Finish your dose as prescribed
- Don’t share or take shared medications
Check out this CDC video on antifungal resistance in A. fumigatus. www.cdc.gov/aspergillosis/php/guidance/index.html
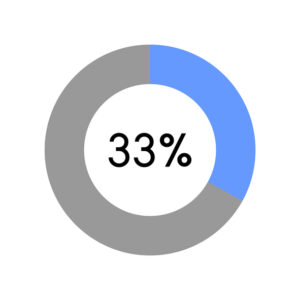
Patients with azole-resistant Aspergillus fumigatus infections are 33% more likely to die, compared with patients with Aspergillus fumigatus infections that can be treated with azoles.
TREATMENT OPTIONS
In this section, we go over the drugs and other treatments used to manage aspergillosis, with a brief discussion of investigational therapies as well. Prior to the introduction of the triazole antifungals, amphotericin was the recommended therapy for invasive aspergillosis. You will notice that it is the drug that was used as the comparator in many of the older studies.
We have arranged the drugs in alphabetical order by class of drug because sometimes your doctor will recommend switching the antifungal drug class or combining classes of drugs when the first treatment is not effective. While polyenes were the first class of agents used for aspergillosis, triazoles were found effective and safe and are now generally recommended first. But polyenes and even drugs belonging to the class echinocandins are also options for patients who can’t take triazoles or aren’t responding to them.
It’s important to note that we provide generalizations about these therapies. Your provider will work with you to determine the best course of therapy for you. Your provider will consider the type of Aspergillus you have, your medical history, and other factors such as kidney function, other medicines you are taking, and whether you are pregnant or breastfeeding when selecting your therapy.
While all of the drugs listed below are FDA-approved, some are not specifically approved to treat Aspergillus infection but are discussed in the Infectious Diseases Society of America Aspergillus Guidelines.
Finally, all of the data discussed are related to management of invasive aspergillosis in adults. Information for pediatric patients is coming in a later module.

Triazoles
Triazoles are the most commonly used drugs for invasive aspergillosis. Many of these medicines can be provided both by mouth and vein. They are named by their chemical structure. Azoles can interact with a lot of medications, so your provider will need to consider all the medications you are taking when starting azole therapy. The FDA-approved azoles are listed first.
FDA-approved Triazole Therapies
Isavuconazonium sulfate (CRESEMBA®)
HOW IT IS GIVEN: By vein (intravenous) and by mouth (capsules)
APPROVAL STATUS: FDA approved for invasive aspergillosis
HOW WELL IT WORKS: Isavuconazonium sulfate was found to be non-inferior to (not worse than) voriconazole (VFEND) in the management of invasive aspergillosis. Here is more information about this study.
COMMON SIDE EFFECTS: Vomiting, nausea, diarrhea, liver problems, electrolyte problems, shortness of breath, swelling of arms or legs, back pain, and headache
FINANCIAL RESOURCES: CRESEMBA® Support Solutions. Call 1-800-477-6472 or visit the Support Solutions Page.
For patient information, see the Cresemba website.
Itraconazole (SPORANOX®, ONMEL®, suba-itraconazole, TOLSURA®)
HOW IT IS GIVEN: By mouth, capsule, or oral solution
APPROVAL STATUS: FDA-approved for aspergillosis in the lung or elsewhere in patients who can’t take or haven’t responded to amphotericin B. This drug is also commonly used for allergic and chronic aspergillosis conditions.
HOW WELL IT WORKS: In a small study, itraconazole was found effective for management of invasive pulmonary aspergillosis that did not respond to amphotericin B.
SIDE EFFECTS: Vomiting, diarrhea, abdominal pain, dizziness, drowsiness, rash, headache, blurred vision, liver damage, joint pain, heart problems, and swelling. It also has a number of drug-drug interactions.
Posaconazole (NOXAFIL®)
HOW IT IS GIVEN: By vein (IV) or by mouth (delayed-release tablets or an oral suspension)
APPROVAL STATUS: FDA approved for invasive aspergillosis
HOW WELL IT WORKS: Posaconazole works as well as voriconazole for invasive aspergillosis and is well tolerated. To learn more, read this article.
SIDE EFFECTS: Gastrointestinal side effects (abdominal pain, constipation, diarrhea, nausea, vomiting), fever, swelling, low blood count, and liver enzyme elevations
FINANCIAL RESOURCES: NOXAFIL® Merck Patient Assistance Program. Call 800-727-5400 or visit www.merckhelps.com/NOXAFIL
Voriconazole (VFEND®)
HOW IT IS GIVEN: By vein (IV) or by mouth (tablets or suspension)
APPROVAL STATUS: Voriconazole is FDA approved for the management of invasive aspergillosis.
HOW WELL IT WORKS: Voriconazole worked better than conventional amphotericin B as initial therapy and had fewer severe side effects. Read here to learn about this study.
SIDE EFFECTS: Visual disturbances, nerve problems, liver problems, heart rhythm problems, bone problems, and interactions with other drugs, long-term use: skin sensitivity and skin cancer

Polyenes
These drugs are derivations of amphotericin B and are named for their chemical structure. At this time, these drugs must be given by vein, but a version that can be delivered by mouth is being studied (See Clinical Trials).
Amphotericin B Deoxycholate (conventional amphotericin, FUNGIZONE®), IV
HOW IT IS GIVEN: By vein (intravenous)
APPROVAL STATUS: FDA approved for invasive fungal infections such as aspergillosis
HOW WELL IT WORKS: Amphotericin B deoxycholate was the gold standard therapy for aspergillosis before triazoles. It is rarely used anymore because the lipid forms are safer for the kidneys. To learn more, click here and here.
SIDE EFFECTS: Fever, low blood pressure, upset stomach, loss of appetite, vomiting, diarrhea, anemia, kidney damage, and liver damage, allergic reaction
Amphotericin B lipid complex (ABLC, ABELCET®), IV
HOW IT IS GIVEN: By vein (intravenous)
APPROVAL STATUS: ABLC is indicated for the treatment of invasive fungal infections in patients who are refractory to or intolerant to conventional amphotericin B.
HOW WELL IT WORKS: In a study conducted in patients with multiple invasive fungal infections, 42% of patients with aspergillosis experienced a complete or partial response to ABLC.
SIDE EFFECTS Chills, fever, kidney problems, organ failure
FINANCIAL SUPPORT: Leadient Biosciences Patient Assistance Program: 800-490-3262
Liposomal amphotericin B (AmBisome®)
HOW IT IS GIVEN: Through your vein (intravenous)
APPROVAL STATUS: Approved for patients with Aspergillus species refractory to amphotericin B deoxycholate or in patients with renal impairment or unacceptable toxicity precludes the use of amphotericin B deoxycholate
HOW WELL IT WORKS: In a study across fungal infections (including aspergillosis), liposomal amphotericin B was used successfully in patients with documented aspergillosis. Read more about this study here.
SIDE EFFECTS: Rash, high blood sugar, electrolyte abnormalities, nausea, vomiting, low blood count, liver function abnormalities, chills, trouble sleeping, kidney function abnormalities and shortness of breath
Echinocandins
Echinocandins are medications given by vein that inhibit the synthesis of part of the fungal cell wall. These drugs are typically used as alternatives to azoles or as part of a combination approach.
Anidulafungin (Eraxis®)
HOW IT IS GIVEN: By vein (intravenous)
APPROVAL STATUS: Not approved for invasive aspergillosis, but it is listed in the 2016 Aspergillus IDSA guidelines with a caution that the data are limited.
HOW WELL IT WORKS: Found more effective when used in combination with voriconazole vs voriconazole alone. To learn more about this study, read this.
SIDE EFFECTS: Low blood pressure, high blood pressure, shortness of breath, blood clots, blood electrolyte problems, liver function abnormalities, trouble sleeping
Caspofungin (Cancidas®)
HOW IT IS GIVEN: By vein (intravenous)
APPROVAL STATUS: FDA approved for treatment of invasive aspergillosis in patients who have not responded to or can’t tolerate other therapies (i.e., amphotericin B, lipid formulations of amphotericin B, or itraconazole)
HOW WELL IT WORKS: Was found effective in 45% of patients as the second therapy for invasive aspergillosis. To learn more about this study, click here.
SIDE EFFECTS: Not common: Fever, complications in the vein where the drug was infused, nausea, vomiting, flushing, abnormalities in liver function, other laboratory test abnormalities
Micafungin (Mycamine®)
HOW IT’S GIVEN: By vein (intravenous)
APPROVAL STATUS: Micafungin is not FDA approved for invasive aspergillosis. It is recommended in the IDSA guidelines as an option after initial therapy fails (salvage therapy).
HOW WELL IT WORKS: Non-randomized studies in patients with invasive aspergillosis and patients with low white cell counts from chemotherapy suggest that micafungin works as well as other antifungal therapies. To learn more about the data on micafungin for invasive aspergillosis, review this paper.
SIDE EFFECTS: Diarrhea, agitation, headache, black stools, breathing problems, decreased urination, belly pain, tiredness, and bleeding or bruising
Rezafungin (Rezzayo®)
HOW IT IS GIVEN: By vein (intravenous)
APPROVAL STATUS: Not FDA-approved for invasive aspergillosis
HOW WELL IT WORKS: Not established in clinical studies, but rezafungin does have potent activity against a range of Aspergillus spp (in laboratory studies). To learn more about this study, click here. Because of once weekly dosing, it may have an advantage for use in combination approaches.
SIDE EFFECTS: Flushing, warm sensations, hives, nausea, tightness in the chest (infusion reaction), sensitivity to the sun, and abnormal liver tests
Clinical Trials and Investigational Agents

Clinical trials are research studies that test how well new treatment approaches work. They have an important place in your care as researchers strive to improve current aspergillosis treatments and search for new and better ones. Clinical trials are essential for learning about the management of invasive aspergillosis.
Our most effective antifungal treatments would not be available without the clinical trial process. Unfortunately, many people with aspergillosis, or their loved ones, are unaware of the option for a clinical trial or are unsure about the value of participating.
Your goal is to find the best treatment available whenever you make a treatment decision. While there may be a good standard of care for you or your loved one—care that experts believe is appropriate for your specific diagnosis and treatment history—sometimes the current standard of care is not as effective as you and your healthcare team would like. Other times, the standard of care works for a time but then stops working. In still other instances, there is no standard of care for your situation. Participation in a clinical trial may be the best option for you.
The best time to search for clinical trials is every time you are faced with a treatment decision.
At the time this website has been developed, these are some promising therapies in development for invasive aspergillosis:
- Olorofim is an oral drug that belongs to a novel class of drugs called orotomides. This drug has good activity against a variety of Aspergillus spp. It can penetrate the lung, liver, kidney and brain and has low potential for drug-drug interactions. In the FORMULA-OLS study, olorofim had positive outcomes for patients with invasive aspergillosis and limited or no treatment options. To learn more about the results of this preliminary study, look here
- Fosmanogepix is another drug using a unique mechanism of action—this IV and oral drug interferes with an enzyme necessary for fungal adherence. It also has broad activity against a number of Aspergillus species, alone and in combination with liposomal amphotericin B. A small study that was stopped in 2022 showed promising results in invasive mold infections. A larger study is launching at the time of this writing
- Ibrexafungerp belongs to a new class called the triterpenoid class, which has some similarities to echinocandins but with lower rates of cross-resistance. This drug interferes with the building of the fungal cell wall. Already FDA-approved for vulvovaginal candidiasis treatment and prevention, ibrexafungerp showed favorable responses in a study conducted in patients with refractory fungal diseases, including those with invasive aspergillosis. It’s also being studied in combination with voriconazole specifically for patients with invasive aspergillosis
- Opelconazole is a triazole drug specifically designed for inhalation therapy. Inhalation therapy for invasive pulmonary aspergillosis is appealing because it gets the drug to the areas needed with fewer side effects and drug-drug interactions. Opelconazole is active against a number of Aspergillus species. It has been studied as prophylaxis against aspergillosis and is being studied in combination with other systemic drugs in refractory invasive aspergillosis
- MAT2203 is an oral and non-toxic encochleated form of amphotericin B (CamB). Encochleation means that the drug is wrapped up in fat-based crystals and calcium that protect the drug from getting broken down within the GI tract. Encochleation also allows the drug to be taken up into the bloodstream and released in tissue because of calcium differences. At the time of this writing, a study is planned with MAT2203 after IV amphotericin B therapy for patients who can’t tolerate azoles (the ORALTO trial).
Surgery

Sometimes surgery is needed to manage various forms of invasive aspergillosis. These include:
- Invasive aspergillosis in the sinuses or the eye
- Invasive aspergillosis in the lungs not responding to treatment
- Aspergilloma (fungus ball) (if possible) when the patient is symptomatic, particularly if coughing up blood
- Endocarditis (in combination with antifungal therapy) with replacement of infected valves if necessary
- Osteomyelitis
- Septic arthritis
- Skin lesions when there are burns or a lot of soft tissue wounds.
Supportive Care: This includes measures to support the body’s functions, such as oxygen therapy, IV fluids, and treatment of any underlying conditions. In some cases, growth factors and other immune stimulation drugs can be considered to support neutrophil levels and fight the fungus.
Questions to ask your doctor about treatment for aspergillosis
- Have you diagnosed invasive aspergillosis? If so, where is it?
- Do you know the genus/species?
- Have you performed antifungal susceptibility testing? If not, is this something that you can obtain?
- What drug are you going to use first?
- How do I take that medication?
- For how long will I have to take that medication? Will you have to make any changes?
- Will this drug interact with any of my other medications?
- How do you know if the medication is working?
- What are the side effects?
- What is the cost of the medication? How will you help me with insurance?
- What will we do if it does not work?
- Will I need any other treatments? (e.g., surgery)?
![]()